Bone metabolism
Introduction
Bone tissue is in a constant state of remodeling: resorption of old bone and formation of new bone. A proper balance between both processes is crucial for bone health. This delicate equilibrium is tightly regulated and influenced by multiple factors such as physical exercise, hormonal status, and nutrient and vitamin availability. Under normal conditions, 5-10% of our total bone volume is renewed per year1.
This article exposes the mechanism of bone remodeling and the main factors that regulate it: hormones, nutrients and physical exercise.
Bone composition and properties
Bone is a highly vascularized tissue composed of bone cells embedded in a mineralized organic matrix, which consists mainly of hydroxyapatite (Ca₁₀(PO₄)₆(OH)₂), responsible for its stiffness, and collagen fibers, which contribute to its resilience2. This combination makes bones hard to deform but not fragile. Regarding its cells2:
- Osteoblasts promote bone formation by the synthesis of collagen and other components of the extracellular matrix.
- Osteocytes derive from osteoblasts. In particular, osteoblasts differentiate to osteocytes when they get trapped in the newly synthesized bone matrix. They are responsible for the mechanotransduction of bone (its response to mechanical signals).
- Osteoclasts are responsible for bone resorption, resulting in the breaking down of the tissue and the release of calcium and phosphate to the bloodstream. This process is essential in a healthy bone: it allows for the removal of old and damaged bone and its adaptation to new mechanical loads (bones can change shape depending on how they are used).
Remodeling process
The remodeling cycle relies on a close coordination between cells and signaling pathways. It follows these steps3:
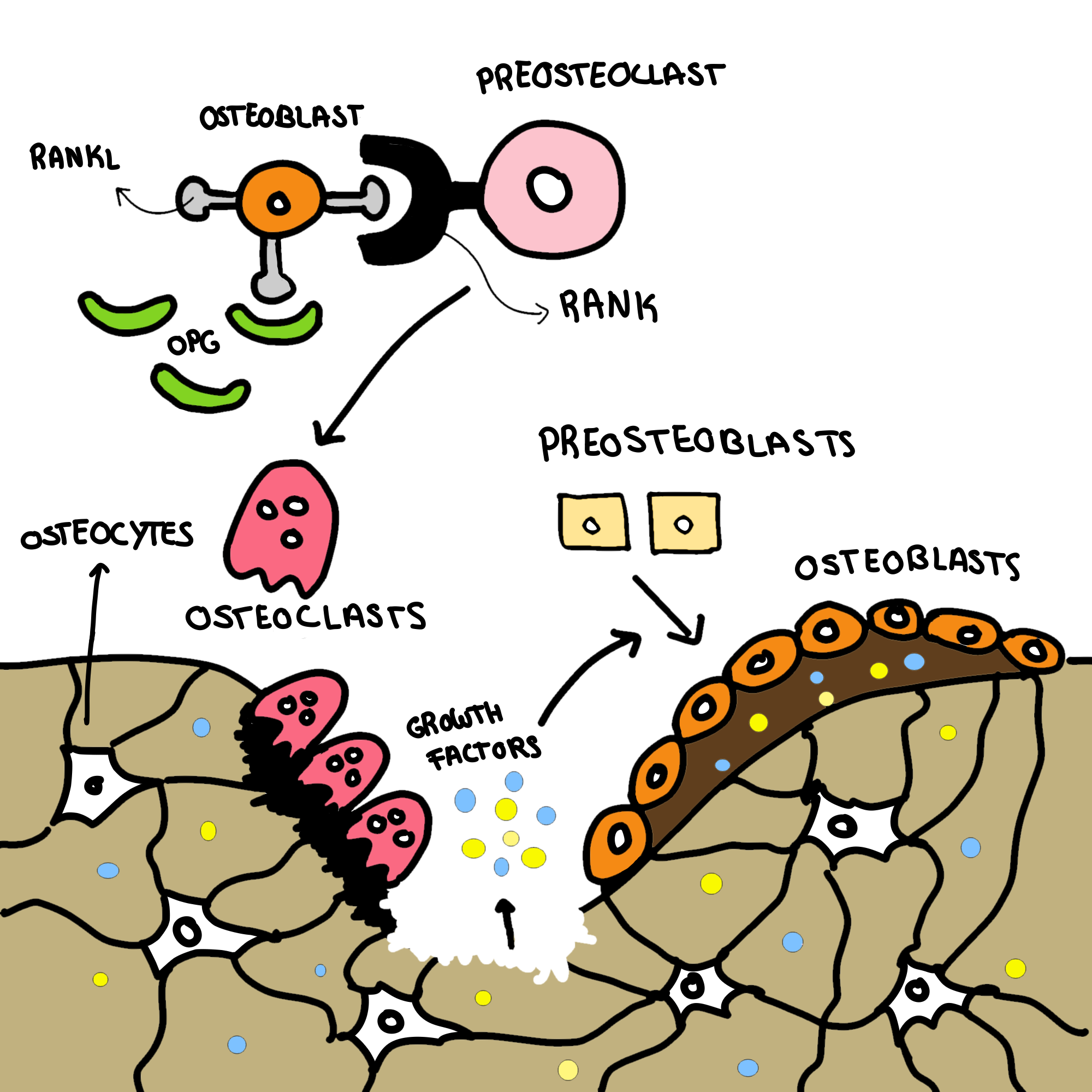
Recruitment of preosteoclasts to the target bone area and differentiation into mature, active osteoclasts.
Lytic activity of osteoclasts and the consequent destruction of bone. This process releases growth factors that were trapped in the bone matrix, such as transforming growth factor beta (TGF-β) and insulin-like growth factor I (IGF-I), which then recruit preosteoblasts.
Recruitment of preosteblasts and differentiation into active osteoblasts, which synthesize new bone. IGF-I and TGF-β are secreted and become integrated into the newly formed bone matrix. Some osteoblasts differentiate into osteocytes, others interact with preosteoclasts triggering the cycle.
Bone remodeling regulation
The recruitment of osteoclasts is regulated primarily by osteoblasts. Osteoblasts express RANK ligand (RANKL) on their membrane surfaces, which interacts with RANK, a receptor on osteoclasts membranes. This binding triggers the differentiation of preosteoclasts into active osteoclasts. However, osteoblasts also produce osteoprotegerin (OPG), which competes with RANK for the binding to RANKL, decreasing the activation of osteoclasts. Therefore, the RANKL/OPG ratio is an indicator of the physiological balance of bone remodeling. A high ratio (RANKL>OPG) favors resorption (for example, at the beginning of the cycle), and a low ratio (OPG>RANK) corresponds to inhibited resorption and a bone formation phase3.
In addition, osteocytes produce sclerostin, a protein that inhibits osteoblast activity decreasing bone formation4.
Influence of hormones
Bone health is conditioned by the proper functioning of the hormonal system. The main hormones that interfere are:
Estrogens: sex steroid hormones, abundant in females, which promote bone growth by increasing the number and function of osteoblasts and stimulating their production of OPG. Estrogen decline during menopause is tightly associated to bone loss and the development of osteoporosis5.
Parathyroid hormone (PTH): secreted by the parathyroid glands in response to hypocalcemia, stimulating bone resorption and the release of calcium into the bloodstream1.
Calcitonin: synthesized by the C cells of the thyroid in response to hypercalcemia. It inhibits bone resorption by reducing the number and activity of osteoclasts1.
Calcitriol (active form of vitamin D): vitamin D, obtained through sun exposure or diet (eggs, fatty fish…) is transformed into calcitriol, a hormone that promotes calcium and phosphate absorption in the intestines, crucial for bone mineralization. It also promotes the activity of osteoclasts, but overall it supports bone formation1.
Influence of nutrients
Calcium is indispensable for the mineralization of bone. More than 99% of the body’s calcium is stored in the skeleton, forming hydroxyapatite. Maintaining optimal calcium levels is also crucial for other vital functions, such as muscle contraction. If our dietary calcium intake is insufficient, PTH secretion increases, leading to enhanced bone resorption1.
Sun exposure or vitamin D intake is also required for a proper bone mineralization as described in the previous section.
Influence of physical exercise
Osteocytes are able to sense mechanical stimulus, reducing sclerostin synthesis and promoting bone growth. Consequently, physical exercise is highly recommended to preserve bone mass4.
Conclusion
Bone metabolism is a complex process that involves the coordination of osteoblasts, osteoclasts and osteocytes, regulated by hormones such as PTH, calcitonin, estrogens and calcitriol. Sun exposure, regular physical exercise and adequate calcium intake can help us keep our bones healthy and prevent bones disorders such as osteoporosis.